Why Am I Not Getting Pregnant Even Though All My Tests Are Normal?
By Deanna Thomas, Lead Practitioner, Acupuncture & Wellbeing, Middlesbrough BSc (Hons) Acupuncture · Lic.Ac · MBAcC · CNHC Registered · PG Diploma Obstetrics & Gynaecology · Advanced training in reproductive immunology and male fertility
You've done what you were told to do. You've tracked your cycle. You've had the bloods, the scans, maybe the HSG. Your partner has had a semen analysis. Everyone keeps saying everything looks fine, perfectly normal, nothing to worry about. And yet. Month after month, you're still not pregnant. If you're searching this question at 11pm with a sinking feeling in your chest, please know this first: you are not imagining it, and you are not alone.
Here's the honest answer. Standard fertility tests confirm the absence of obvious problems. They do not confirm the presence of optimal fertility. There is a real and often substantial gap between "normal" and "ideal", and that gap is where many couples in your position find themselves. Roughly one in seven UK couples experience difficulty conceiving, and around a quarter of those receive an "unexplained" diagnosis, which simply means current standard testing did not find a cause. It does not mean there is nothing happening. It means we have not looked deeply enough yet.
At our clinic in Middlesbrough we work with women and couples from across Teesside who arrive in exactly this position. They have been told everything is fine, but their bodies are quietly telling a different story. This post will walk you through what "normal" actually means, what standard tests often miss, what you can do this week, and how a different lens, including fertility acupuncture in Middlesbrough, can help fill in the picture.
Key Takeaways
- "Normal" on a fertility test means within an accepted reference range, not optimal for conception. The two are not the same thing.
- Standard NHS testing rarely covers sperm DNA fragmentation, full thyroid panels, fertility-optimal ferritin levels, microbiome status, or mid-luteal progesterone timed correctly to your actual cycle length.
- Day 21 progesterone is only the right test day for a 28-day cycle. For longer or shorter cycles, the test must be timed to 7 days after ovulation or the result is misleading.
- NHS "normal" ferritin starts around 15 ng/mL. Fertility-aware ranges are generally 40 to 50 ng/mL or higher, and lower ferritin has been linked to higher risk of ovulatory infertility.
- The vaginal and endometrial microbiome can significantly affect implantation, even when every standard test looks fine. It is not part of NHS investigation but is increasingly available privately.
- Egg maturation takes around 90 days and sperm regeneration takes around 72 to 74 days. This is the window in which preconception preparation has its biggest impact.
- Acupuncture has measurable effects on uterine blood flow and parasympathetic nervous system activity, two mechanisms directly relevant to conception when standard tests are unrevealing.
The frustration that brings you to this question
Most women I see arrive carrying a very particular kind of weight. They have done their research. They have followed the advice. They have heard "just relax" from people who have no idea how exhausting that suggestion is. They are not anxious, hysterical, or overthinking it. They are intelligent, tuned-in women who can feel, with quiet certainty, that something is not adding up.
If that sounds like you, please trust that instinct. Your body is not lying to you. The tests are simply not designed to answer the question you are actually asking, which is not "is anything visibly broken?" but "why isn't conception happening?" Those are different questions. Standard testing answers the first one. The second one usually requires a wider lens.
What "normal" really means on a fertility test
When a result comes back as "normal", what that actually means is that your number falls inside a statistical reference range built from a broad population. That range is wide. It is designed to flag clear problems, not to identify subtle imbalances or to define what is optimal for you, in your body, at this point in your life.
A simple example. Many fertility-relevant hormones have reference ranges that span three to four times the lower limit. A result at the lower end of "normal" and a result at the upper end of "normal" are technically both fine. In practice, they can produce very different cycles. The same applies to thyroid function, vitamin D, ferritin, and progesterone. Two women can both be "normal" and still have very different fertility pictures.
This is the first thing to understand. Normal is a yes-or-no flag. Optimal is a different conversation entirely.
What standard NHS fertility testing usually does not include
NHS fertility investigation is excellent at ruling out the big, structural, identifiable issues. It is not designed to be exhaustive, and that is not a criticism, simply a reality of how a population-level service works. A typical workup for a heterosexual couple in the UK includes day 21 progesterone, day 2 to 5 FSH and LH, sometimes AMH, sometimes a basic TSH, a pelvic ultrasound, possibly an HSG, and a semen analysis covering count, motility, and basic morphology.
What that workup typically does not look at:
- Sperm DNA fragmentation. A man can have a perfectly "normal" semen analysis and still have high levels of DNA damage in his sperm. A 2019 meta-analysis published in Fertility and Sterility found that male partners of women with recurrent pregnancy loss had significantly higher levels of sperm DNA fragmentation than partners of fertile control women, with a mean difference of nearly 12 percentage points [1]. Standard NHS testing does not measure this.
- Full thyroid panel. A TSH alone often misses subclinical thyroid issues. Free T3, Free T4, and thyroid antibodies can show patterns that affect ovulation, implantation, and miscarriage risk even when TSH itself looks fine.
- Vitamin and mineral status. Low vitamin D, low ferritin, low B12, and suboptimal omega-3 levels are all linked to fertility outcomes. They are rarely tested as standard.
- Ovulation quality, not just presence. A day 21 progesterone confirms that ovulation occurred. It does not tell you whether the luteal phase is long enough, whether the egg released was a strong one, or whether the whole second half of the cycle is hormonally supportive of implantation.
- Cycle-wide hormone patterns. Most testing is single-point. A snapshot taken on day 21. Hormones do not work in snapshots, they work in relationships and patterns across an entire cycle.
- Immune and inflammatory factors. Subtle immune dysregulation, chronic low-grade inflammation, and conditions such as endometriosis can affect fertility long before they show up on a routine scan.
None of these are exotic, fringe ideas. They are well-recognised in fertility medicine. They simply sit outside the standard NHS investigation pathway, which is designed to identify the most common, most treatable causes first.
"Normal" is a yes-or-no flag. Optimal is a different conversation entirely.
A pattern I see often at the clinic
Clinical patternA woman in her early thirties arrives with a folder of normal results. Eighteen months of trying. Day 21 progesterone confirms ovulation. Her partner's semen analysis is fine. The GP has been kind and reassuring and has nothing more to offer. On detailed history-taking we find a luteal phase of 9 days, spotting before her period, cold hands and feet, exhaustion by mid-afternoon, and stress that has been quietly chronic for years. None of this lands on a test. All of it shapes the environment in which conception is, or is not, happening.
That pattern is not rare. It is the most common version of "everything is normal but I'm not pregnant" we see at our Middlesbrough clinic. The fix is not dramatic. It is paced, foundational work over the egg and sperm preparation window, supporting the body to do what it already knows how to do.
Three things I see often that didn't show up on standard tests
These are not theoretical. These are the patterns I see across the consultation table at our Middlesbrough clinic, in women whose folder of NHS results says everything is fine. Each one illustrates the same underlying point: tests can be technically "normal" while still missing something that matters for conception.
The "low" progesterone that was tested on the wrong day
This one is so common it's heartbreaking. A woman is sent for a "day 21 progesterone" test to confirm ovulation. The result comes back low. She is told her luteal phase looks weak, or that ovulation is poor, and she leaves with a quietly devastating question mark over her cycle. Then she comes to us and we ask her cycle length. Thirty-two days. Thirty-five days. Twenty-six days. Anything other than the textbook 28-day cycle.
Here is the issue. Day 21 progesterone is only the right day for a 28-day cycle, where ovulation falls around day 14 and progesterone peaks roughly seven days later. For a 32-day cycle, ovulation typically happens around day 18, which means the mid-luteal peak falls around day 25, not day 21. A test on day 21 in this woman would catch progesterone on the way up, well before its peak, and the result will look "low" when in fact her luteal phase may be perfectly healthy. For a 26-day cycle, the correct test day is closer to day 19. The test itself isn't wrong. The timing was.
If your cycles are not a textbook 28 days, ask for your progesterone test to be timed to seven days after your ovulation, not blindly on day 21. If you are tracking ovulation with LH strips or BBT, you can date this yourself. This single correction has rewritten the diagnosis for several women I've worked with.
The "normal" ferritin that wasn't fertility-optimal
NHS ferritin "normal" ranges typically start somewhere around 15 ng/mL. That range was built to flag clinical iron deficiency anaemia, not to define optimal iron status for ovulation, egg quality, or healthy implantation. Fertility-aware practitioners and reproductive endocrinologists generally look for ferritin of at least 40 to 50 ng/mL, ideally higher, before they would consider iron status truly supportive of conception.
This isn't a fringe idea. A large prospective study of more than 18,500 women, drawn from the Nurses' Health Study II at Harvard, found that women who took iron supplements had a 40% lower risk of ovulatory infertility than women who did not [7]. A ferritin of 22 ng/mL might be perfectly "normal" by NHS reporting, while sitting well below what a body trying to conceive would actually want. It's a classic case of normal not meaning optimal.
The vaginal and endometrial microbiome nobody tested
This is one of the newer pieces of the fertility picture, and it is genuinely changing how we understand unexplained difficulty. The reproductive tract has its own microbial community, and when that community is dominated by Lactobacillus species, implantation and pregnancy outcomes are significantly better. When it shifts away from Lactobacillus dominance, the endometrium becomes a less hospitable environment for an embryo, even when every other test looks normal.
A landmark 2016 study published in the American Journal of Obstetrics and Gynecology found that women with a non-Lactobacillus-dominated endometrial microbiota had implantation rates of 23.1% compared with 60.7% in women with a healthy Lactobacillus-dominated one, and live birth rates of 6.7% compared with 58.8% [6]. Those are not small differences. The vaginal and endometrial microbiome is not part of standard NHS fertility investigation, but it is increasingly available privately, and for women with unexplained difficulty or recurrent implantation issues, it is worth knowing about.
Beyond the bloods: the quieter factors that affect conception
Even with a perfect set of test results, conception relies on a long, beautifully orchestrated chain of events. Egg quality. Cervical fluid. Timing. Tubal pickup. Fertilisation. Cell division. Implantation. Hormonal support of the early embryo. Many of these stages cannot be tested directly. They can only be supported indirectly, by looking after the body that is doing all of the work.
Egg and sperm quality take time to shift
This is one of the most empowering pieces of information I share with new fertility clients. Egg maturation takes approximately 90 days, and sperm regeneration takes approximately 72 to 74 days. That means the egg you ovulate this month, and the sperm that meets it, were both being prepared roughly three months ago. What was happening in your life and your partner's life back then, the sleep, the stress, the nutrition, the inflammation, the alcohol, the heat exposure, the cycle quality, all of that has shaped this month's fertility window.
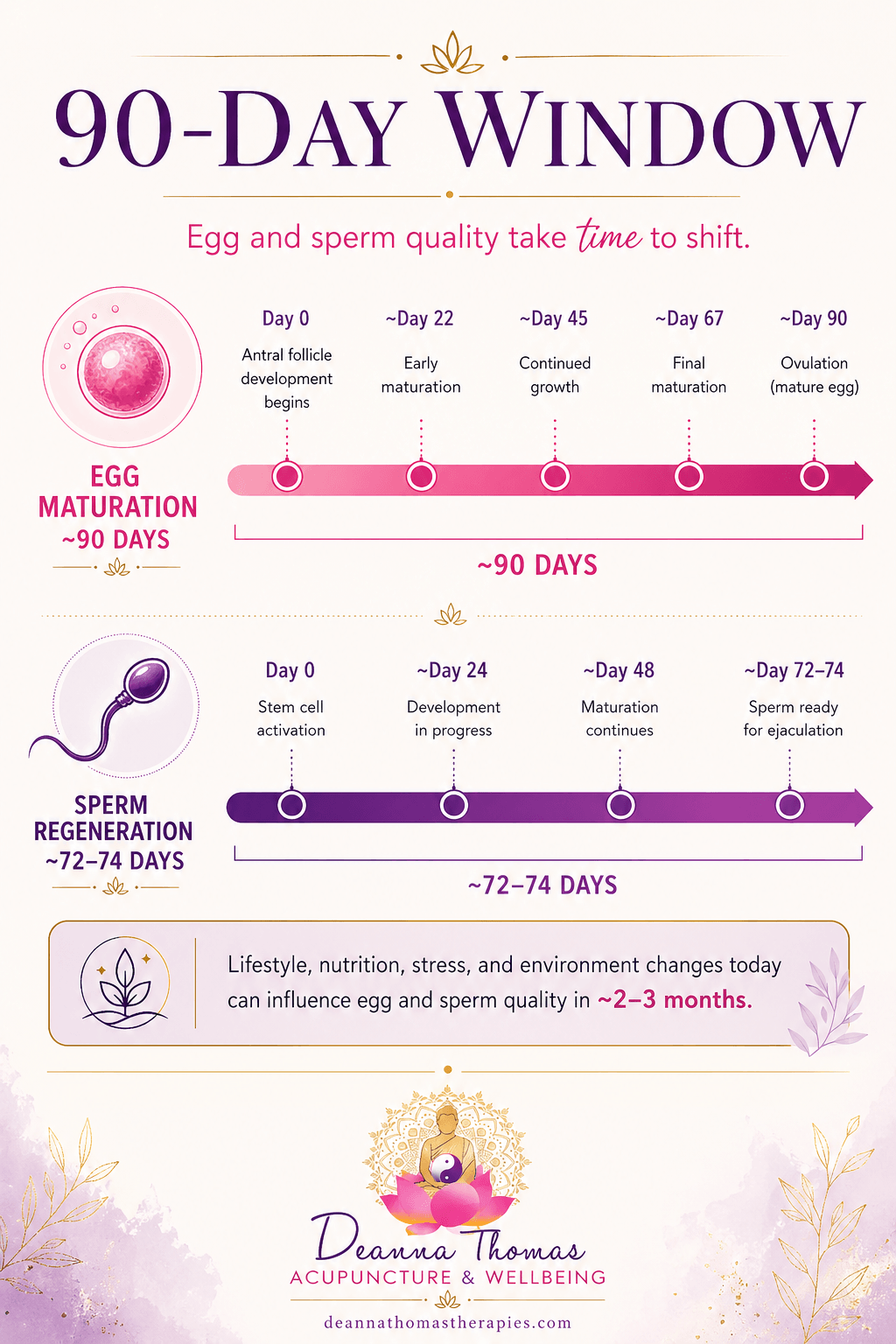 The 90-day window: lifestyle, nutrition, and stress changes you make today shape the quality of eggs and sperm 2 to 3 months from now.
The 90-day window: lifestyle, nutrition, and stress changes you make today shape the quality of eggs and sperm 2 to 3 months from now.This is also why preconception care has to be measured in months, not weeks. It is one of the reasons we ask clients to commit to a course of treatment rather than a single session. The window of preparation is the window of change.
Stress, sleep, and the nervous system
I do not say "just relax", because I know how dismissive that sounds and because the research is more nuanced than that simple instruction suggests. What we do know is that the body's stress response, the sympathetic nervous system, directly competes with reproductive function. When the body perceives ongoing strain, whether from work, grief, fertility worry itself, poor sleep, or chronic over-functioning, it prioritises survival over reproduction. That is biology, not weakness.
How acupuncture can help when tests look normal
Acupuncture is most useful here as a regulating, supportive therapy that works on the whole system. It is not a single-issue intervention. It is a way of bringing the body back to a more balanced, well-resourced state, which then supports better reproductive function. Two specific mechanisms are worth naming, because both are directly relevant when standard tests have come back unrevealing.
Improving blood flow to the uterus
One of the most cited studies in fertility acupuncture, published in Human Reproduction in 1996 by Stener-Victorin and colleagues at the University of Gothenburg, showed that electroacupuncture significantly reduced the pulsatility index in the uterine arteries of infertile women, which is a clinical measure of uterine blood flow impedance [2]. The effect persisted 10 to 14 days after the treatment course ended. Better blood flow to the uterus supports endometrial development and implantation, which is one of the more practical reasons fertility acupuncture is used in the lead-up to a treatment cycle or natural conception attempt.
Calming the nervous system
Acupuncture's most consistent and well-documented effect is its impact on the autonomic nervous system. Research published in Medical Acupuncture in 2020 showed that acupuncture stimulation produced a measurable, transient increase in parasympathetic nervous system activity, captured through the high-frequency component of heart rate variability [3]. In plain language, acupuncture nudges the body out of "stress mode" and into "rest, digest, and repair" mode. For many women in the "everything is normal but I'm not pregnant" position, that nervous system regulation is the missing piece.
Supporting natural conception more broadly
A 2024 scoping review and meta-analysis published in Frontiers in Endocrinology looked specifically at acupuncture for infertility resulting in natural conception (rather than IVF). The pooled data showed acupuncture was significantly more effective than human chorionic gonadotrophin (HCG) for inducing pregnancy across 11 randomised trials, and outperformed no treatment in achieving pregnancy [4]. The authors note that more high-quality research is still needed, which is honest, but the overall direction of evidence is encouraging.
Honest about the wider evidence picture
It's worth being clear that the evidence base on acupuncture for fertility has evolved considerably in recent years, and not every review has reached the same conclusion. Earlier systematic reviews, particularly on acupuncture during IVF cycles, found inconsistent benefit. More recent and much larger analyses have been more positive. A May 2025 Bayesian network meta-analysis of 96 randomised trials involving 14,736 women undergoing IVF or embryo transfer, published in the Journal of Assisted Reproduction and Genetics, found that acupuncture-related therapies, particularly when started months before egg retrieval, were associated with higher clinical pregnancy and live birth rates [5]. The certainty of the evidence remains low to moderate, which the authors are upfront about. The honest position is that the picture is more nuanced than any single study can capture, the direction of more recent and larger evidence is encouraging, and acupuncture is best offered as supportive care alongside, never instead of, appropriate medical investigation.
I want to be honest about what acupuncture is not. It is not a guarantee. It is not a quick fix. It is not a substitute for proper medical investigation when that is indicated. What it is, is a steady, evidence-informed way of supporting the conditions in which conception is more likely to happen.
Three things you can do this week
Before your next appointment, before any further investigation, here are three things you can start now. None of them require permission from anyone.
- Track your basal body temperature for one full cycle. A simple BBT thermometer and a free app. This single piece of information tells you more about ovulation timing, luteal phase length, and overall cycle quality than most of the bloods you've already had.
- Map your cycle symptoms in detail. Length of bleed, colour of flow, clotting, cramps, spotting, cervical fluid, sleep quality, mood, energy. This is information no test can capture and every clinician worth their salt will want to see.
- Have an honest conversation with your partner about the next 90 days. Sleep, alcohol, sauna and hot tub use, stress, exercise. Sperm regeneration takes 72 to 74 days, so changes made this week show up in the sperm being made for two to three months from now.
Tests to consider asking your GP about
If you've been trying to conceive for 12 months or more (or 6 months if you're 35 or over) and your standard results are normal, these are the tests it can be reasonable to ask your GP about. Some are NHS-available, some may require private testing, and some your GP may push back on. Knowing they exist puts you in a stronger position to ask.
- Sperm DNA fragmentation test (sometimes called SCSA, TUNEL, SCD, or Halo): not part of standard semen analysis but increasingly recognised as relevant in unexplained difficulty and recurrent loss.
- Full thyroid panel: TSH, Free T3, Free T4, and thyroid antibodies (TPO and TG), not just TSH alone.
- Vitamin D, ferritin, B12, and folate. If your cycles are regular but you are still not pregnant, ferritin is particularly worth asking about. NHS "normal" starts at around 15 ng/mL but fertility-aware ranges are generally 40 to 50 ng/mL or higher. Ask for the actual number, not just whether it's "normal".
- Mid-luteal progesterone with proper timing. Ideally 7 days after confirmed ovulation, not blindly on day 21, which is only correct for a textbook 28-day cycle. If your cycle is longer or shorter, the test day must shift accordingly or the result is misleading.
- AMH and antral follicle count: a fuller picture of ovarian reserve than FSH alone.
- Prolactin and a fasting glucose / HbA1c: particularly relevant if there are any cycle irregularities or symptoms suggestive of insulin resistance.
- Vaginal or endometrial microbiome testing (private, e.g. Igenomix EMMA / ALICE / EndomeTRIO or similar): worth considering if you have had repeated unexplained difficulty or implantation issues. Not standard NHS but increasingly recognised.
None of this is a substitute for proper medical guidance. It's a starting point for a more thorough conversation with your GP or a fertility specialist.
What we do at the clinic when "everything is normal"
When someone arrives at our Middlesbrough clinic with a folder of normal results and a quiet, persistent sense that something is being missed, the first thing we do is take a properly long history. Not a 15-minute slot. A full consultation. Cycle, symptoms, sleep, digestion, history, lifestyle, partner factors, emotional landscape, the lot.
From there, we usually look at three things together: the patterns the body is showing, whether further investigation might be useful, and what a realistic, paced support plan looks like. Usually a four-month commitment to fertility acupuncture support and lifestyle work, with three months mapped to the egg and sperm preparation window and a fourth to give the prepared cycle a real chance to do its job.
For couples in this position, we offer the Natural Fertility Programme™, which is built specifically for those trying to conceive naturally without ART. (Roots To Transfer™ is a separate programme for couples already in or approaching IVF.) Individual results vary, of course, and we will never pretend otherwise. With more than 800 five-star reviews across Fresha and Google, we are one of very few clinics in the North East that routinely includes both partners in the consultation. In our experience, treating fertility as a couple, where there is a couple, tends to support a more complete picture than treating one person alone.
Frequently Asked Questions
How long should I keep trying before I push for more investigation?
NHS guidance is generally to seek further investigation after 12 months of trying without conception, or after 6 months if you are 35 or over. If your tests have come back normal but you are still not pregnant after 12 to 18 months, it is reasonable to ask for a referral to a fertility specialist for a deeper look, including more advanced sperm analysis, additional hormonal investigation, or imaging. Trust your instincts. You know your body.
My day 21 progesterone came back low. Does that mean I'm not ovulating properly?
Not necessarily. Day 21 progesterone is only the correct test day for a textbook 28-day cycle. If your cycle is longer or shorter, day 21 will be the wrong day. For a 32-day cycle, mid-luteal is around day 25; for a 26-day cycle, around day 19. A "low" result simply caught progesterone before its peak, not a luteal phase defect. Ask your GP to repeat the test 7 days after your actual ovulation, ideally tracked with LH strips or basal body temperature, before drawing any conclusions.
Could my partner's "normal" semen analysis be hiding something?
Yes, this is a very real possibility. A standard semen analysis looks at count, motility, and basic morphology. It does not measure sperm DNA fragmentation, which research now links to recurrent pregnancy loss and reduced fertility outcomes even when the basic semen parameters are within normal range. If you have been trying for 12 months or more with normal results, asking about a sperm DNA fragmentation test (SCSA, TUNEL, SCD, or Halo) is a reasonable next step.
Which programme is right for me, Natural Fertility or Roots To Transfer?
If you are trying to conceive naturally and not currently in or imminently approaching IVF, the Natural Fertility Programme™ is designed for you. If you are preparing for an IVF or FET cycle, or already mid-treatment, Roots To Transfer™ is the right path. If you're not sure where you sit, a consultation will clarify it quickly.
Is acupuncture worth trying when I haven't been given a clear diagnosis?
This is actually one of the situations where acupuncture can be most useful, because it works on the whole system rather than targeting a single diagnosed issue. When standard testing has not given you a clear answer, a regulating, supportive approach that improves blood flow, calms the nervous system, and supports cycle quality often gives the body what it has been missing. We always recommend acupuncture alongside, not instead of, appropriate medical care.
How long does acupuncture take to make a difference?
Most fertility clients work with us across a minimum of four months. Three of those months are mapped to the natural egg and sperm preparation window, and the fourth gives the prepared cycle the conditions in which conception can actually take place. Some couples conceive within the first cycle of treatment. For others, particularly where there are layered factors, the work takes longer. We commit to a course of treatment rather than single sessions because, biologically, this is the timescale on which fertility actually shifts.
Final Thoughts
If your tests have come back normal but month after month you are still not pregnant, you are not failing and you are not imagining the problem. You are running into the limits of what standard testing can see. Your body is not the test. There is almost always more to the story, and very often there is something that can be done about it.
The women and couples we work with across Middlesbrough, Yarm, Stockton, and the wider Teesside area arrive in this exact place, and they leave with something they did not have before: a clearer picture, a paced plan, and the steady, evidence-informed support of our fertility acupuncture service alongside them.
You don't have to navigate this alone. Support is here if and when you're ready.
Explore Fertility SupportAbout the Author
Deanna Thomas · BSc (Hons) Acupuncture · Lic.Ac · MBAcC · CNHC Registered · PG Diploma Obstetrics & Gynaecology
Deanna is the lead practitioner at Deanna Thomas Acupuncture & Wellbeing in Middlesbrough, specialising in fertility, IVF support, women's health, and menopause. She holds a postgraduate diploma in Obstetrics and Gynaecology and has completed advanced training in reproductive immunology and male fertility, equipping her to look beyond standard fertility testing for couples whose results have been told to be "normal". The clinic has more than 800 five-star reviews across Google and Fresha and was named Three Best Rated 2026 and Fresha Highly Recommended 2026.
References
- McQueen DB, Zhang J, Robins JC. Sperm DNA fragmentation and recurrent pregnancy loss: a systematic review and meta-analysis. Fertility and Sterility. 2019;112(1):54-60.e3. DOI: 10.1016/j.fertnstert.2019.03.003
- Stener-Victorin E, Waldenström U, Andersson SA, Wikland M. Reduction of blood flow impedance in the uterine arteries of infertile women with electro-acupuncture. Human Reproduction. 1996;11(6):1314-1317. DOI: 10.1093/oxfordjournals.humrep.a019378
- Kitagawa Y. Spectral Analysis of Heart Rate Variability During Trigger-Point Acupuncture of Various Muscles. Medical Acupuncture. 2020;32(3):150-156. DOI: 10.1089/acu.2020.1414
- Tian Z, Zhang C, Liao X, et al. Trends in acupuncture for infertility: a scoping review with bibliometric and visual analysis. Frontiers in Endocrinology. 2024;15:1351281. DOI: 10.3389/fendo.2024.1351281
- Bin C, Zhong H, Zhang S, et al. Effects of acupuncture-related therapies on pregnancy outcomes among women undergoing in vitro fertilization and embryo transfer: a Bayesian network meta-analysis. Journal of Assisted Reproduction and Genetics. 2025;42(6):1925-1938. DOI: 10.1007/s10815-025-03489-3
- Moreno I, Codoñer FM, Vilella F, et al. Evidence that the endometrial microbiota has an effect on implantation success or failure. American Journal of Obstetrics and Gynecology. 2016;215(6):684-703. DOI: 10.1016/j.ajog.2016.09.075
- Chavarro JE, Rich-Edwards JW, Rosner BA, Willett WC. Iron intake and risk of ovulatory infertility. Obstetrics and Gynecology. 2006;108(5):1145-1152. DOI: 10.1097/01.AOG.0000238333.37423.ab
Citations verified via PubMed.